




















































 Loading ...
Loading ...
Don’t buy an intraoral scanner for dental 3D printing until you read this!
Summary: Consumers need to pay close attention to how an intraoral scanner performs in terms of trueness and precision as this will influence the outcome of the dental 3d printing digital workflow. Results from three studies conducted by Dr. George Michelinakis show that direct digitalization via an intraoral scanner was more accurate than indirect digitalization via CBCT scan for the production of additively manufactured models. However, some scanners tend to have lower trueness when scanning posteriors and tend to deviate more as a scan progresses distally. For complete arch restorations, it is essential to be aware of the accuracy of an intraoral scanner.

Figure 1 - Measuring trueness of Medit i500 IOS.
Introduction
One of the fundamental qualities of an intraoral scanner (IOS) is its accuracy - the sum of trueness and precision. International Standard Organisation 5725 defines trueness as the ability of a measurement or measuring device (such as dental software) to match the actual value of the quantity being measured. Precision is the ability of a measurement or measuring device to consistently repeat a particular measurement. When examining the performance attributes of a particular IOS device a consumer needs to pay close attention to how the scanner performs in terms of trueness and precision both in vitro and in vivo. This will influence the outcome of the dental 3d printing digital workflow.
Accuracy of Intraoral Scanners vs CBCT Devices
In a study published in the European Journal of Prosthodontics and Restorative Dentistry, Dr. Michelinakis looked into the clinical trueness of the 3Shape TRIOS IOS when scanning intact dentition of 20 patients and how this trueness is influenced by the position of the teeth (anterior/posterior, left/right) and the jaw (maxilla/mandible).

Silicone impressions for reference were taken and the resulting gypsum models were scanned with a high accuracy lab scanner to serve as controls against which the IOS scans were compared. The same gypsum models were also scanned with Planmeca’s ProMax 3D Mid CBCT device to compare against the IOS files displayed in dental software. The TRIOS IOS demonstrated a statistically significant (t(39)=-2.4, p=0,019) higher trueness for the anterior teeth (41,8μm, SD 16.2) compared to the posterior (47,0μm, SD 16.3).
Figure 2 - TRIOS trueness between anterior and posterior teeth.

Results did not show any statistically significant difference on TRIOS IOS trueness between maxillary and mandibular teeth or between left and right quadrants. When direct digitization with the TRIOS IOS was compared against indirect digitization of plaster models using the Planmeca CBCT device, the results indicated a statistically significant difference in trueness between the two methods of digitization (z =4.36, p <0,005). Median IOS full arch trueness was 38,6μm whereas median CBCT full arch trueness was 61,7μm.
Figure 3 - IOS scan is statistically more accurate compared to an
indirect CBCT scan of plaster models.
The clinical significance of these findings for direct IOS scanning is that the posteriors are scanned with lower trueness because of the difficulty in reaching these areas of the mouth, especially with a scanner that has a large tip like the TRIOS 2 used in this study. Regarding the comparison between direct IOS scan and indirect CBCT scan of plaster models, results indicated that the direct method of digitization was statistically more accurate, therefore the production in dental software of an additively manufactured resin model should be done using direct scan data.
Accuracy when scanning a complete arch
In an in vitro study published in 2020 Dr. Michelinakis worked with a research team to examine the accuracy of three different IOS devices when scanning a complete arch. 38 gypsum models were scanned with the 3Shape TRIOS 3, the Medit i500 and the Planmeca Emerald IOS devices. The same models were also scanned by a high accuracy lab scanner to provide reference files. The research team investigated a number of parameters that contribute to accuracy such as trueness, precision and the ability of scanners to reproduce without over- or underestimation of the reference scanner’s file size.
A significant difference was found among the scanners regarding trueness (F (2.37)=239.7, P<.001). The complete arch trueness of the Planmeca Emerald(56.6μm) was significantly lower than either the Medit i500 (15.8μm) or the 3Shape TRIOS 3 (16.8μm)(both P<.001). No significant difference in trueness was revealed between the Medit i500 and the 3Shape TRIOS 3 scanners (P=.365).

Figure 4 - Complete arch trueness of three different IOS devices.


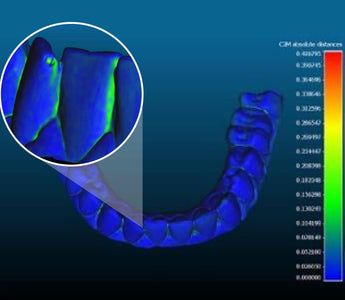
Figure 5 - Measuring complete arch trueness of 3Shape TRIOS 3 IOS (left) and Planmeca Emerald IOS (right).


Figure 6 - Visualizing trueness (zooming in on anterior segment) of 3Shape TRIOS 3 IOS (left) and Planmeca Emerald IOS (right).
One important finding is how some scanners tend to deviate more as the scan progresses distally and also in the interdental embrasures, especially in the case of mal-aligned teeth.
A significant difference was found among the scanners regarding precision (F (2.89) = 301.2, P<.001). 3Shape’s TRIOS 3 scanner was significantly more precise than the other two scanners (P<.001) while the Planmeca Emerald scanner was significantly more precise than the Medit i500 scanner (P<.001) which produced files that significantly underestimated the reference scanner files (t(37)= -12.4, P<.001). The other scanners did not significantly underestimate or overestimate the files of the reference scanner (t(37)= 1.91, P=.062 for the 3Shape TRIOS 3 and t(37)= 1.64, P=.101 for the Planmeca Emerald) even though it became apparent that the Planmeca Emerald had the largest variability of all. These findings are important to take into account when an IOS is used for scanning for complete arch restorations.

Figure 7 - Estimation of reference file size according to IOS.
Influence of Material Substrates on Accuracy
In an in vitro study published in 2022, Dr. Michelinakis’ research team investigated the effect that different scanning substrates have on the accuracy of three different IOS devices. The team used a typodont model with nine different substrates to investigate how dental substrates and materials with different refractive indices influence the way light from an IOS is reflected onto their surface and how this can influence scanning accuracy.

Figure 8 - Typodont model with different substrate materials.
The typodont was scanned with the 3Shape TRIOS 3, the Carestream 3600 and the Planmeca Emerald S scanners for test files, and with a high accuracy lab scanner for reference files.
Results indicated that material translucency and reflectiveness influenced the scanning accuracy of the scanners tested.
The reflective metal crown was scanned with lower trueness produced by all three scanners, with the Emerald S showing the greatest deviation. Reducing light reflection from the restoration surface by spraying it with titanium dioxide was shown to reduce maximum scanning deviations.
In this study, decreasing the light reflection by sandblasting the surface of a typical Class II occlusal-mesial extended amalgam restoration did not result in significantly different scanning trueness compared to the polished Class II amalgam restoration of the same size, regardless of the scanner used.

Translucent materials (such as Emax and incisal composites) were scanned more accurately with the Trios3 IOS (confocal microscopy technology) compared to the Carestream 3600 IOS (active triangulation data acquisition technology). Translucent materials such as enamel-shaded composites and lithium disilicate seem to negatively impact active triangulation IOS devices’ accuracy more compared to confocal microscopy IOS’.
Figure 9 - IOS effect on different substrate trueness.
There was a statistically significant difference in the performance of the three intraoral scanners for complete arch trueness. Pairwise comparisons revealed that TRIOS 3 had a significantly higher trueness compared to CS3600 (P=.000) and Emerald S (P=.000) while the complete arch trueness of CS3600 and Emerald S did not differ significantly (P=.393).

The results of complete arch precision of the three intraoral scanners were also significantly different (χ2=7.091, P=.029). The precision was statistically significantly different between TRIOS 3 and CS3600 (P= .044), and between TRIOS 3 and Emerald S (P=.044), but not between CS3600 and Emerald S (P=.286).
Figure 10 - Complete arch trueness and precision for the 3 IOS tested.
Conclusion
Accuracy significantly influences the outcome of a dental 3d printing digital workflow when using an intraoral scanner. Three studies conducted by Dr. George Michelinakis made several conclusions on the accuracy and effectiveness of selected intraoral scanners. One study found that trueness was not influenced by the position of teeth, with no statistically significant difference between maxillary and mandibular teeth, or between quadrants. Another study found significant differences in trueness and precision between three types of IOS scanners. The most recent study indicated that material substrate translucency and reflectiveness influenced the scanning accuracy of scanners tested.
Once a user has determined the right intraoral scanner for their practice, they can begin to adopt a comprehensive dental 3d printing solution that will enhance their productivity and make patient visits more efficient while retaining high quality outcomes. Ackuretta’s 3D Printing Solution offers users a convenient and streamlined dental 3d printing workflow, including AI-supported slicing dental software, 3d printers, washers, and uv curing ovens. Once users have scanned with an intraoral scanner and designed an application using dental software, Ackuretta’s solution enables a calibrated and integrated workflow from slice to cure for maximum productivity and high quality dental 3d printing.
_________________________________________________
George has received a Degree in Dental Science by the National and Kapodistrian University of Athens, a MSc in Fixed and Removable Prosthodontics, a MPhil in Fixed and Removable Prosthodontics at the University of Manchester Dental School and Hospital UK, and completed a 3-year training programme in the specialty of Prosthodontics. Since 2004 he has maintained a private practice in Greece specializing in Prosthodontics and Implant Dentistry. He has published in both English and Greek dental journals, authored a chapter in a book published by Quintessence, lectured in numerous national and international conferences and serves as a reviewer for acclaimed prosthodontic journals.




